Along with all aspects of life, there are risks related to viruses and the vaccines that are designed to protect us from those viruses. For a majority of the population, many studies strongly suggest that the benefits of vaccine far outweighs the risks of vaccine.
Since there are reasonable perceptions that mRNA vaccines have insufficient long-term safety data, and there are known concerns about mRNA manufacturing purification processes, and all vaccines have demonstrated adverse events and death in very healthy people at low-risk of severe COVID-19, optimal (lower) dosing options and boost timing, specific to physiology / risk / “weight” categories should be developed and available as options to the low-COVID-risk population to encourage vaccine acceptance and maximize safety ~Primum non nocere. While it is not possible nor pragmatic to expect elimination of all vaccine risks, it likely that optimizations of dose and schedule could make the vaccine vs COVID risk enticing to the entire population, even those who have recovered from natural infection.
Balancing the Efficacy and Safety of Vaccines in the Elderly
With advances in global health care, ageing populations are expected to grow worldwide throughout the 21[st] century. Increased lifespan is a testament to modern medical and social practices, but also presents a growing challenge to a system with limited …
Safety of High Doses of Influenza Vaccine and Effect on Antibody Responses in Elderly Persons
Background Immune responses after influenza immunization are reduced in elderly individuals, the group at greatest risk for complications and death after influenza. Improved vaccines are needed to address this problem.Methods Ambulatory individuals 65 years and older (N = 202) were…
Vaccination in the elderly: The challenge of immune changes with aging
The unprecedented increase of life expectancy challenges society to protect the elderly from morbidity and mortality making vaccination a crucial mean…
Ischaemic stroke and influenza A H1N1 vaccination: a case report
We report a 75-year-old male patient who suffered posterior circulation ischaemia after influenza A/H1N1 vaccination. Vaccination provokes a variable magnitude of inflammatory and immunological response that modifies the risk for ischaemic stroke. Whereas …
[Local reaction and neutralization test in smallpox vaccination after previous inoculation with MVA. Stickl’s graduated vaccination (author’s transl)] – PubMed
Of 200 first inoculations and 8 revaccinations, the sera were examined for content of neutralizing vaccine antibodies 3 weeks after the MVA graduated inoculation. In spite of imponderables which affect the failure rate in the “clinical trial”, a positive result was obtained on first vaccination in 8…
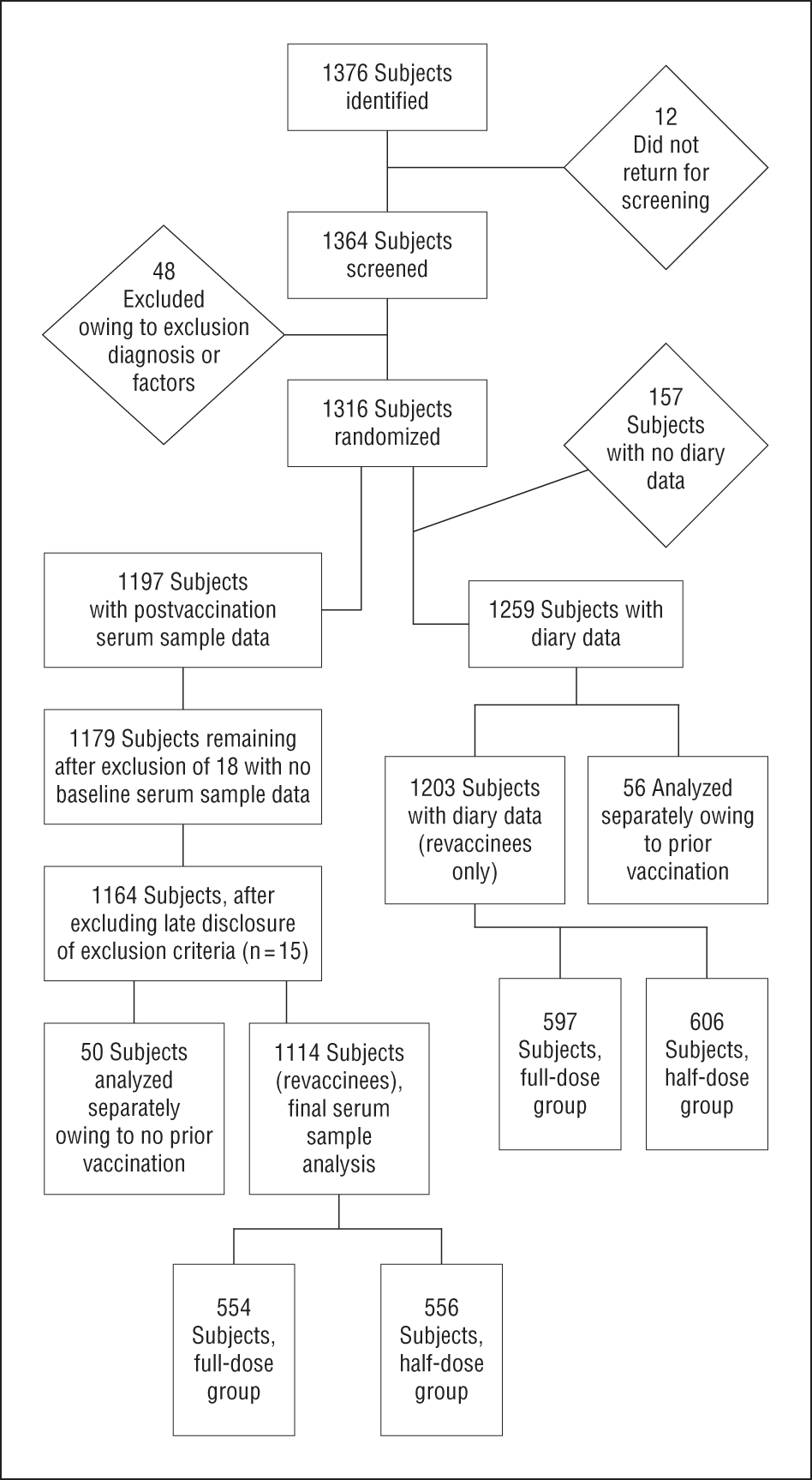
Half- vs Full-Dose Trivalent Inactivated Influenza Vaccine (2004-2005)
Background Optimal public health strategies for managing influenza vaccine shortages are not yet defined. Our objective was to determine the effects of age, sex, and dose on the immunogenicity of intramuscular trivalent inactivated vaccine (TIV).Methods Healthy adults aged 18 to 64…
A Reduced-Dose Seasonal Trivalent Influenza Vaccine Is Safe and Immunogenic in Adult and Elderly Patients in a Randomized Controlled Trial
With the recent pandemic of influenza A (H1N1) and vaccine shortages, there has been considerable interest in developing influenza vaccines with reduced doses, allowing for increased production capacity. Here we report a prospective, randomized, double-blind, …
What are the side effects of COVID-19 vaccines, and should you worry?
In this feature, we look at the side effects of each of the 13 COVID-19 vaccines that have been authorized for use in at least one country.
Reactions and Adverse Events of the Pfizer-BioNTech COVID-19 Vaccine | CDC
Information about reactions and adverse events reported by recipients of the Pfizer-BioNTech COVID-19 Vaccine
The Vaccine Adverse Event Reporting System (VAERS) Results
Processing Request, please wait for results…
Waldenstrom’s Disease: Symptoms, Diagnosis, and Treatments
Waldenstrom’s macroglobulinemia is rare type of non-Hodgkin lymphoma. This disease’s symptoms, treatment, and outlook vary.
European Scientists Zero In On AstraZeneca Blood Clot Link
A rare blood clotting condition has occurred in some people after receiving the AstraZeneca COVID-19 vaccine. If the new research is correct, it could mean that blood clots could be easily treated.
Platelet antibodies of the IgM class in immune thrombocytopenic purpura – PubMed
The clinical course and response to therapy of patients with immune thrombocytopenic purpura (ITP) are not completely determined by the level of IgG present on the platelet surface. It is possible that antibodies of other immunoglobulin classes also play a role in platelet destruction in some of the…
From Europe: 3,964 People Have Died from Adverse Drug Reactions for COVID-19 “Vaccines” – 162,610 Injuries
Thousands of Europeans have been injured and have died from taking the COVID-19 (China coronavirus) vaccine since it was first distributed to the public. A database maintained in Europe has an inventory of cases where people either died or were injured from the China coronavirus vaccines. The list i…
Fact Check-Deaths reported under UK ‘Yellow Card’ scheme aren’t confirmed to be linked to COVID-19 vaccination
Social media posts have claimed that more than four hundred people have died soon after receiving the coronavirus vaccine. This claim needs context.
COVID-19 Vaccination
COVID-19 vaccines protect against COVID-19. Get safety info and more.
Covid-19: Norway investigates 23 deaths in frail elderly patients after vaccination
Doctors in Norway have been told to conduct more thorough evaluations of very frail elderly patients in line to receive the Pfizer BioNTec vaccine against covid-19, following the deaths of 23 patients shortly after receiving the vaccine. “It may be a coincidence, but we aren’t sure,” Steinar Madsen…
Acute Allergic Reactions to mRNA COVID-19 Vaccines
This study examines the incidence of acute allergic reactions to mRNA COVID-19 vaccine administrations in health care employees in Massachusetts.
Cutaneous Reactions Reported after Moderna and Pfizer COVID-19 Vaccination: A Registry-Based Study of 414 Cases
Cutaneous reactions after mRNA-based COVID-19 vaccines have been reported but are
not well characterized.
COVID-19 toes, Moderna arm, all-body rash: Vaccines can cause skin reactions but aren’t dangerous, study says
A new study finds some COVID-19 vaccine skin reactions, including a measles-like rash and shingles, are rare, and thankfully brief, side effects.
Dick’s Sporting Goods Park vaccine site closes early after 13 patients experience adverse reactions
The mass vaccination site at Dick’s Sporting Goods Park in Commerce City was shut down early Wednesday after people started having adverse reactions to the Johnson & Johnson COVID-19 vaccine.…
No evidence the COVID-19 vaccine caused Hank Aaron’s death | PolitiFact
A spokesperson at the Fulton County Medical Examiner’s office confirmed that Aaron died of natural causes and that his death was not linked to the COVID-19 vaccine.
‘Healthy’ South Florida doctor died 2 weeks after receiving COVID-19 vaccine
MIAMI BEACH, Fla. (CBS12) — A 56-year-old doctor passed away this week two weeks after getting his first dose of a Pfizer COVID-19 vaccine. Dr. Gregory Michael, a Miami-Beach obstetrician, was in good health, according to WPDE. Health officials from Florida and the Centers from Disease Control…
Utah woman, 39, dies 4 days after 2nd dose of COVID-19 vaccine; autopsy now completed
SALT LAKE CITY (KUTV) — During a KUTV investigation into COVID-19 vaccine side effects and where to report them, we found four reported deaths, filed by Utah families and their caregivers to the CDC’s Vaccine Adverse Effects Reporting System. UPDATE:Utah’s Office of the Medical Examiner …
Health care worker dies after second dose of COVID vaccine, investigations underway
Tim Zook, a resident of Orange who worked at an acute care medical center, fell ill within hours of his second Pfizer-BioNTech shot. He spiraled downward and died four days later.
COVID immune response suspected in young doctor’s death
Dr. J. Barton Williams did not know he had COVID; antibody was present in his blood, doctors say.
Overdose reactions could help show what may happen to those more sensitive to normal doses and <30 day dose timing.
Hamilton man recovering after receiving accidental double second dose of COVID-19 vaccine
Victor Smith, 91, received his second dose of the Moderna vaccine last week. He was accidently given another dose four hours later and became ill.
Coronavirus: German care home workers accidentally given vaccine overdose | DW | 28.12.2020
An oversight has led to eight care workers at a residential home on the north German coast receiving five times the recommended dose of the vaccine. Four were taken to hospital after developing flu-like symptoms.
How LVHN Colleagues Feel After Second Dose of COVID-19 Vaccine
BY KATIE CAVENDER When you receive a COVID-19 vaccine, your immune system goes to work creating antibodies to protect itself from the coronavirus. The vaccine CANNOT cause a COVID-19 infection but can cause side effects, including pain at the injection site, tiredness, headache, muscle pain, chills,…
I felt totally fine after my first COVID-19 shot, but the second dose was rough. Here’s a timeline of my side effects and why I still think you should get the shot.
Dr. Joy Henningsen says she felt muscle aches and soreness six hours after getting the Pfizer shot, but felt almost back to normal 48 hours later.
More Side Effects for Second Doses of COVID-19 Vaccine
The second dose of COVID-19 vaccines can cause stronger side effects than the first. Fatigue, headache and muscle pain may effect 40-50% of people.
Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine | NEJM
Correspondence from The New England Journal of Medicine — Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine
VERIFY: What happens if I get the 1st dose of the COVID-19 vaccine but delay the 2nd?
The second coronavirus vaccine dose is about building memory within your body, so there isn’t a ‘waiting too long’ period as recognized by the CDC.
Administration of a Second Dose of the Moderna COVID-19 Vaccine After an Immediate Hypersensitivity Reaction With the First Dose: Two Case Reports | Annals of Internal Medicine
Background: In December 2020, the U.S. Food and Drug Administration issued an emergency use authorization for the Pfizer-BioNTech and Moderna messenger RNA vaccines for the prevention of COVID-19. This authorization was a significant step toward mitigating the burden of the disease. Nevertheless, hy…
This news article data has not been verified, but it is interesting to see that in younger people, risk of COVID-19 vs risk of vaccine may be similar.
For 25 year olds: Risk of COVID-19 related death: 23 in 1 million Risk of serious harm due to side-effects: 11 in 1 million
Covid-19 vaccines: What’s happening to unused jabs?
Surplus vaccine doses are piling up in some countries while others say they are not getting enough.
Winton Centre Cambridge
Winton Centre for Risk and Evidence Communication
Putting risks into context: covid-19 vaccines and blood clots – The BMJ
The media around the world have been desperate to help put the risks of blood clots following a covid-19 vaccination into some sort of context. It’s a familiar issue: every […]More…
Think Twice Before Giving the COVID Vax to Healthy Kids
Based on the data to date, there’s no compelling case for it right now
Senator Johnson, families speak: COVID vaccine adverse reactions
Some people report the COVID-19 vaccines led to serious side effects – and Sen. Ron Johnson (R-Wisconsin) hosted a few of them in Milwaukee on Monday, June 28.
Two die in Japan after shots from suspended Moderna vaccines – Japan govt
Two people died after receiving Moderna Inc COVID-19 vaccine shots that were among lots later suspended following the discovery of contaminants, Japan’s health ministry said on Saturday.
Michigan boy dies 3 days after getting Pfizer COVID-19 vaccine, CDC is investigating
The CDC is investigating the case of a 13-year-old Saginaw County boy who died three days after getting his second dose of a COVID-19 vaccine.
It’s abundantly clear the many ways the CDC misrepresented the data on children. https://t.co/KEKyj23lFV









 Loading…
Loading…


















/cloudfront-us-east-2.images.arcpublishing.com/reuters/Z5L7EJOVJJIE3NNOVL4EFMYDKU.jpg)

