COVID-19 is presenting as many diseases. Acute Respiratory Distress Syndrome and the treatment for ARDS is likely NOT the correct treatment. There is a hemoglobin attack and oxygen deprivation component that is possibly more important to understand and treat than any associated pneumonia related components. The information below comes from various medical professionals who are trying desperately to identify good solutions. Currently it appears that steroids are proving very helpful as noted in the first several links below. Also see COVID-19 Therapeutics and Hospitalized Patient Physical Therapy.
Is short half-life Budesonide, Ciclesonide, and similar Inhaled Corticosteroids (ICS) an optimal treatment in some cases? Do they help increase pulse-oximeter measured blood oxygen saturation levels? Should it be administered on a calendar or physiologic event basis?
Could a rapid acting short-half-life steroid eliminate need for oxygen supplement long enough to begin [monoclonal / polyclonal] antibody (Regeneron) therapy?
Corticosteroid inhalers used by asthma patients may help treat COVID-19, researchers to begin human clinical trials – Health News , Firstpost
The ultimate goal of the trial is to analyse if the Budesonide inhaler can be used as a low-cost and easily available early intervention therapy for COVID-19 patients to reduce the risks of severe respiratory illness.
“The primary outcome was defined as COVID-19-related urgent care visits, including emergency department assessment or hospitalisation.”. “In the per-protocol analysis, the primary outcome occurred in ten (14%) participants in the usual care group and one (1%) participant in budesonide group (difference in proportions 0·131, 95% CI 0·043–0·218; p=0·004), indicating a relative risk reduction of 91% for budesonide.” “This effect, with a relative reduction of 91% of clinical deterioration is equivalent to the efficacy seen after the use of COVID-19 vaccine“
Inhaled budesonide in the treatment of early COVID-19 (STOIC): a phase 2, open-label, randomised controlled trial
Early administration of inhaled budesonide reduced the likelihood of needing urgent
medical care and reduced time to recovery after early COVID-19.
Inhaled budesonide in the treatment of early COVID-19 illness: a randomised controlled trial
Background Multiple early hospital cohorts of coronavirus disease 2019 (COVID-19) showed that patients with chronic respiratory disease were significantly under-represented. We hypothesised that the widespread use of inhaled glucocorticoids was responsible for this finding and tested if inhaled gluc…
Inhaled corticosteroids: A rapid review of the evidence for treatment or prevention of COVID-19 – The Centre for Evidence-Based Medicine
Laura C Armitage and Rachel Brettell On behalf of the Oxford COVID-19 Evidence Service Team Centre for Evidence-Based Medicine,
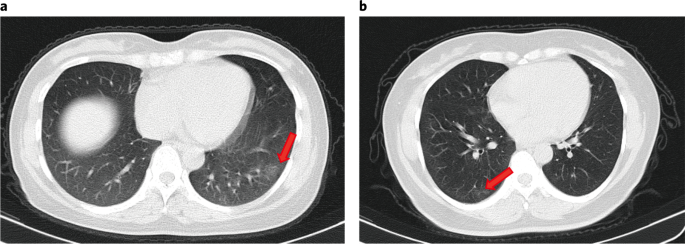
Therapeutic potential of ciclesonide inhalation for COVID-19 pneumonia: Report of three cases
No specific and effective anti-viral treatment has been approved for COVID-19 so far. Systemic corticosteroid has been sometimes administered to severe infectious diseases combined with the specific treatment. However, as lack of the specific anti-SARS-CoV-2 …
Local doctor believes he has found ‘silver bullet’ for COVID-19
“What I’m using is Budesonide, it’s an inhaled steroid that doesn’t have the side effects of total body steroids but it has the benefits.”
Asthma inhalers being trialed for treatment of COVID-19
Researchers from Queensland University of Technology and Oxford University are working in collaboration to begin human clinical trials of inhaled corticosteroids, commonly used for asthma patients, on patients with COVID-19. The researchers believe that this could be useful for patients with the nov…
QUT and Oxford researchers collaborate on new COVID-19 asthma drug trial
QUT researchers are collaborating with colleagues at the University of Oxford on a UK clinical trial to test common asthma inhalers as a treatment for COVID-19 infection.
Researchers to test asthma drug to treat Covid-19 – Korea Biomedical Review
Local infectious disease specialists said they would evaluate the potential of a…
Covis Pharma B.V. Initiates Phase 3 Clinical Trial of Alvesco (Ciclesonide) Inhaler for the Treatment of COVID-19
/PRNewswire/ — Covis Pharma B.V. today announced the initiation of a Phase 3 clinical study to assess the safety and efficacy of its asthma drug Alvesco…
Two Drugs Show Promise Against COVID-19
Korean researchers have screened 48 FDA-approved drugs against SARS-CoV-2, and found that 2, which are already FDA-approved for other illnesses, seem promising. The FDA approval for other uses would greatly reduce the time needed to gain FDA approval of use in COVID-19. The research is published in …
Nip it in the bud: New study will attack SARS-Cov2 where it multiplies | McGill University Health Centre
RI-MUHC researchers initiate a clinical trial of ciclesonide to possibly prevent mild cases of COVID-19 from worsening
Therapeutic potential of ciclesonide inhalation for COVID-19 pneumonia: Report of three cases
No specific and effective anti-viral treatment has been approved for COVID-19 so far. Systemic corticosteroid has been sometimes administered to severe infectious diseases combined with the specific treatment. However, as lack of the specific anti-SARS-CoV-2 …
The inhaled steroid ciclesonide blocks SARS-CoV-2 RNA replication by targeting the viral replication-transcription complex in cultured cells
Here, we screened steroid compounds to obtain a drug expected to block host inflammatory responses and MERS-CoV replication. Ciclesonide, an inhaled corticosteroid, suppressed replication of MERS-CoV and other coronaviruses, including SARS-CoV-2, the cause of COVID-19, in cultured cells. The effecti…
Is the half-life of Methylprednisolone >18hrs? Is that excessive in some cases? Is a short half-life dose of Budesonide and pause an improved treatment in some cases?
Treatment Protocol – Frontline COVID-19 Critical Care Working Group
We have tweaked the protocol based on the best emerging data; however our core philosophy and approach have not changed. Some have asked why our initial protocol included hydroxychloroquine, the anti-viral drug that was widely touted as a cure for the COVID-19 disease that is caused by the virus. …
Is 6mg/day Dexamethasone the correct treatment? Is the half-life of Dexamethasone >36hrs? When administered daily, is the dose cumulative? Is that excessive in some cases? Were some studies that showed depleted immune titers at terminal related to long-half life steroid cumulative effects? Is a short half-life dose of Budesonide and pause an improved treatment in some cases? A possibly related study “27 COVID-19, 51 septic, 18 critically-ill non-septic (CINS)” In the study, the 51+18 cohorts were screened to avoid “greater than or equivalent to 300 mgs/day of hydrocortisone or other immunosuppressive medications” but the COVID-19 cohort was not screened, implying they could have been hit hard with steroids? No treatment info on the COVID-19 group. So how do we know they were not hit hard with steroid? COVID treatments of 6mg/day dexamethasone is equivalent of 150mg hydrocortisone but longer half-life? >36hrs? So it would accumulate up over days? If that were the treatment (again – no way to know from this publication?) how would that end in 10 to 15 days? Is that too much steroid? Is a short hit and pause a better treatment? Or is this study correct and it’s not cytokine induced inflammation at all? Or ?? Study has patient data in important appendix link: https://insight.jci.org/articles/view/140329/sd/1
COVID-19 – EMCrit Project
CONTENTS Basic biology Infection control Transmission Personal protective equipment (PPE) Diagnosis Signs & symptoms Labs Imaging CXR & CT scan Lung ultrasonography General approach to imaging Bronchoscopy Diagnostic approach for admitted patients Treatment: General protocols ED patients getting adm…
Coronavirus (COVID-19) Update: FDA Authorizes Monoclonal Antibodies for Treatment of COVID-19
The FDA issued an EUA for two monoclonal antibodies to be administered together for treating mild to moderate COVID-19 in adults and pediatric patients.
“We found that diabetes mellitus, body temperature ≥ 37.8°C, peripheral oxygen saturation < 92%, and CK-MB > 6.3 are independent predictors of severe disease in hospitalized COVID-19 patients. Appropriate assessment of prognostic factors and close monitoring to provide the necessary interventions at the appropriate time in high-risk patients may reduce the case fatality rate of COVID-19”
Prognostic Factors for Severe Coronavirus Disease 2019 in Daegu, Korea
Jang JG, et al. J Korean Med Sci. 2020 Apr;35(23):e209. https://doi.org/10.3346/jkms.2020.35.e209
Detectable 2019-nCoV viral RNA in blood is a strong indicator for the further clinical severity
The novel coronavirus (2019-nCoV) infection caused pneumonia. we retrospectively analyzed the virus presence in the pharyngeal swab, blood, and the anal swab detected by real-time PCR in the clinical lab. Unexpectedly, the 2109-nCoV RNA was readily detected …
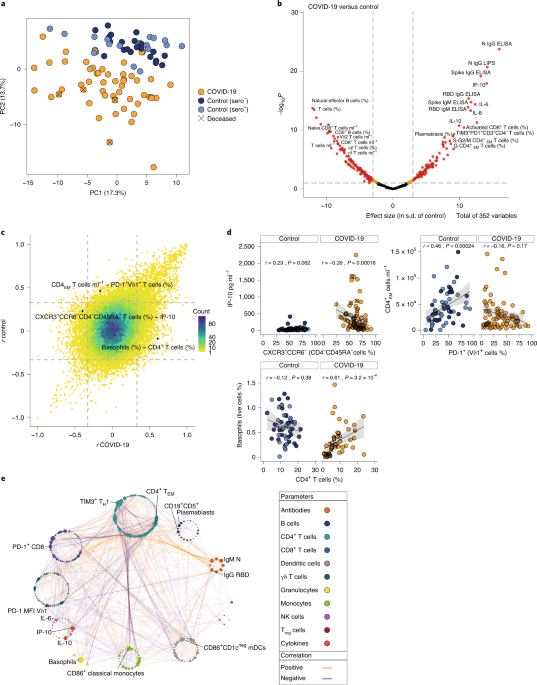
A dynamic COVID-19 immune signature includes associations with poor prognosis
A common immune signature in the blood of patients with COVID-19, who are otherwise clinically heterogeneous, sheds light into the pathogenesis and clinical progression of the disease.
COVID-19 Protocols
Brigham and Women’s Hospital COVID-19 Clinical Guidelines
Kallikrein-kinin blockade in patients with COVID-19 to prevent acute respiratory distress syndrome
The kinin-kallikrein system is a crucial target for the treatment of COVID-19.
Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections
A cohort of asymptomatic patients infected with SARS-CoV-2 had significantly lower levels of virus-specific IgG antibodies compared to a cohort of age- and sex-matched symptomatic infected patients.
60% Of People Naturally Resistant To SARS-COV2, New Study Reveals
New research suggests majority of people may already have resistance based on previous infections…
Do anti-coagulants help increase pulse-oximeter measured blood oxygen saturation levels?
COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up
Coronavirus disease 2019 (COVID-19), a viral respiratory illness caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), may predispose patients to thrombotic disease, both in the venous and arterial circulations, due to excessive …
COVID-19:Attacks the 1-Beta Chain of Hemoglobin and Captures the Porphyrin to Inhibit Human Heme Metabolism
The novel coronavirus pneumonia (COVID-19) is an infectious acute respiratory caused by the novel coronavirus. The virus is a positive-strand RNA virus with high homology to bat coronavirus. In this study, conserved domain analysis, homology modeling, and molecular docking were used to compare the b…
MUST READ! Research Reveals That COVID-19 Attacks Hemoglobin In Red Blood Cells, Rendering It Incapable Of Transporting Oxygen. Current Medical Protocols Could All Be Wrong! – Thailand Medical News
COVID-19 Research: Findings from a new study released by Chinese researchers , Dr Wenzhong Liu from Sichuan University and Dr Hualan Li from Yibin University has revealed that the Sars-CoV-2 coronavirus attacks hemoglobin in the the red blood cells through a series of cellular actions, that ultimat…
Mechanisms of hypoxemia
Oxygen is an essential element for life and without oxygen humans can survive for few minutes only. There should be a balance between oxygen demand and delivery in order to maintain homeostasis within the body. The two main organ systems responsible for …
This video, being a bit dated from Mar 31, 2020, provides important background information and is a call for action to reduce damage from improper ventilator use including that of over-pressure and premature use.
The effect of SARS coronavirus on blood system: its clinical findings and the pathophysiologic hypothesis. – PubMed – NCBI
PubMed comprises more than 30 million citations for biomedical literature from MEDLINE, life science journals, and online books. Citations may include links to full-text content from PubMed Central and publisher web sites.
Special Report: As virus advances, doctors rethink rush to ventilate
When he was diagnosed with COVID-19, Andre Bergmann knew exactly where he wanted to be treated: the Bethanien hospital lung clinic in Moers, near his home in…
Ventilators are overused for Covid-19 patients, doctors say – STAT
If the iconoclasts are right, putting coronavirus patients on ventilators could be of little benefit to many and even harmful to some.
Great medical professional group discussion from Apr 24, 2020
Ventilator Management of Patients With COVID-19
This JAMA Insights Clinical Update discusses the pathophysiology of SARS-CoV-2–related respiratory failure, distinguishing unique L and H phenotypes and their implications for ventilator strategies and settings.
Partly False: COVID-19 infects the blood, not the lungs
Shared widely on Facebook, posts make the primary claim that COVID-19 is not a disease of the lungs and should be treated with chloroquine, zinc or homeopathic remedies rather than putting patients on ventilators ( https://www.facebook.com/shianne.huninghake.10/posts/646947999210656 ; https://www.facebook.com/sushama.gokhale.58/posts/10158163196431866…
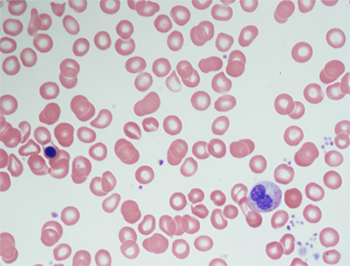
What the blood tests of a COVID-19 patient can tell us
A blood test result typically seen in bone marrow diseases was found in a patient with COVID-19.
COVID-19: All the wrong moves in all the wrong places
In this Editorial, Barrett and Yaffe highlight shortcomings in our collective response to the COVID-19 pandemic and underscore the need for more basic research into this new disease.
Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: an observational study
In the German health-care system, in which hospital capacities have not been overwhelmed
by the COVID-19 pandemic, mortality has been high for patients receiving mechanical
ventilation, particularly for patients aged 80 years or older and those requiring
dialysis, and has been considerably lower for…
Convergent antibody responses to SARS-CoV-2 in convalescent individuals
Convergent antibody responses to SARS-CoV-2 in convalescent individuals
A bridge between life and death: Most COVID-19 patients put on ventilators will not survive
The U.S. is currently facing a shortage of ventilators. Here’s how they work and why they are so important in fighting COVID-19. Just the FAQs, USA TODAY
This is what should be done instead of premature intubation. Solving the red-blood cell problem is a work-in-progress.
How a free, extremely low-risk ER procedure is saving lives from coronavirus
As scientists search for a drug to treat coronavirus, ER doctors are employing a simple, low-risk technique they say is preventing prevent serious infection.
Expert Testimony Before Senate Contradicts Media’s COVID-19 Narrative
Experts testifying in the U.S. Senate provided perspectives on the COVID-19 pandemic that contradicts mainstream coverage of the crisis. by Dennis Behreandt
In the video below, the doctors seemed more credible than Senator Peters at 44min. The doctors and other experts speaking at the following times tend to align best with the research done by Really Correct: 0:48, 1:07. 1:20, 1:27, 1:35. Speakers beyond that have not yet been reviewed. There were speakers not at those mentioned times that may have alternative opinions that are not fully aligned with Really Correct research.
Home Security & Governmental Affairs
May 06, 2020 02:00 PM
Fast Facts on U.S. Hospitals, 2020 | AHA
The American Hospital Association conducts an annual survey of hospitals in the United States. The data below, published in 2020, are a sample from the 2018 AHA Annual Survey (FY 2018).



























 Loading...
Loading...