COVID-19 Therapeutics and Advanced Supportive Care
Therapeutic drugs and other therapies are being aggressively debated, tested, used under compassionate-use expanded access and the like. Below are articles that may be of interest. Really Correct has no strong opinion other than compassionate-use doctor options are good when risks and contraindications are well known or life saving choices are limited. Perhaps obviously, the more severe the case, the less there is to lose when a doctor is trying to save a life with a compassionate-use medical gamble. Also see Severe Treatment and Staying Healthy.
Monoclonal Antibodies
Coronavirus (COVID-19) Update: FDA Authorizes Monoclonal Antibodies for Treatment of COVID-19
The FDA issued an EUA for two monoclonal antibodies to be administered together for treating mild to moderate COVID-19 in adults and pediatric patients.
The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro
Although several clinical trials are now underway to test possible therapies, the worldwide response to the COVID-19 outbreak has been largely limited…
Regeneron’s Casirivimab and Imdevimab Antibody Cocktail for COVID-19 is First Combination Therapy to Receive FDA Emergency Use Authorization | Regeneron Pharmaceuticals Inc.
TARRYTOWN, N.Y. , Nov. 21, 2020 /PRNewswire/ — First treatment of any kind to have prospectively confirmed and statistically significant anti-viral activity against SARS-CoV-2 Authorized for recently diagnosed, mild to moderate COVID-19 in high-risk patients Initial doses of REGEN-COV2 will be
Immunosuppressants, Steroids, Tocilizumab, Cyclosporine A, Etc.
Budesonide – Wikipedia
IUPAC name
Corticosteroid inhalers used by asthma patients may help treat COVID-19, researchers to begin human clinical trials – Health News , Firstpost
The ultimate goal of the trial is to analyse if the Budesonide inhaler can be used as a low-cost and easily available early intervention therapy for COVID-19 patients to reduce the risks of severe respiratory illness.
Ciclesonide – Wikipedia
IUPAC name
UB researchers launch study to learn if an asthma treatment can ease Covid-19
Read the full story from News Reporters Samantha Christmann and Jonathan Epstein.
Covis Pharma B.V. Initiates Phase 3 Clinical Trial of Alvesco (Ciclesonide) Inhaler for the Treatment of COVID-19
/PRNewswire/ — Covis Pharma B.V. today announced the initiation of a Phase 3 clinical study to assess the safety and efficacy of its asthma drug Alvesco…
Dexamethasone – Wikipedia
IUPAC name
Methylprednisolone – Wikipedia
IUPAC name
Methylprednisolone as Adjunctive Therapy for Patients Hospitalized With COVID-19 (Metcovid): A Randomised, Double-Blind, Phase IIb, Placebo-Controlled Trial
AbstractBackground. Steroid use for COVID-19 is based on the possible role of these drugs in mitigating the inflammatory response, mainly in the lungs, trigger
Tocilizumab in patients with severe COVID-19: a retrospective cohort study
Treatment with tocilizumab, whether administered intravenously or subcutaneously,
might reduce the risk of invasive mechanical ventilation or death in patients with
severe COVID-19 pneumonia.
Roche’s Tocilizumab May Not Improve COVID-19 Pneumonia
An Italian study did not observe a benefit for early COVID-19 pneumonia patients who were given tocilizumab, Roche’s RA drug marketed as Actemra.
COVID-19 Outcomes in 4712 consecutively confirmed SARS-CoV2 cases in the city of Madrid.
There is limited information describing features and outcomes of patients requiring hospitalization for COVID19 disease and still no treatments have clearly demonstrated efficacy. Demographics and clinical variables on admission, as well as laboratory markers and therapeutic interventions were extra…
Kallikrein-kinin blockade in patients with COVID-19 to prevent acute respiratory distress syndrome
The kinin-kallikrein system is a crucial target for the treatment of COVID-19.
Read about the use of drugs to reduce blood clot formation in people with COVID-19.
The Role of Anticoagulation in COVID-19-Induced Hypercoagulability
We aim to provide a comprehensive analysis of hypercoagulability in individuals affected by COVID-19. Our goal is to describe the hypercoagulable state related to the infection and provide guidance regarding the possible benefits of anti-coagulation with …
Prevention, Diagnosis, and Treatment of VTE in Patients With Coronavirus Disease 2019
Emerging evidence shows that severe coronavirus disease 2019 (COVID-19) can be complicated
by a significant coagulopathy, that likely manifests in the form of both microthrombosis
and VTE. This recognition has led to the urgent need for practical guidance regarding
prevention, diagnosis, and treatme…
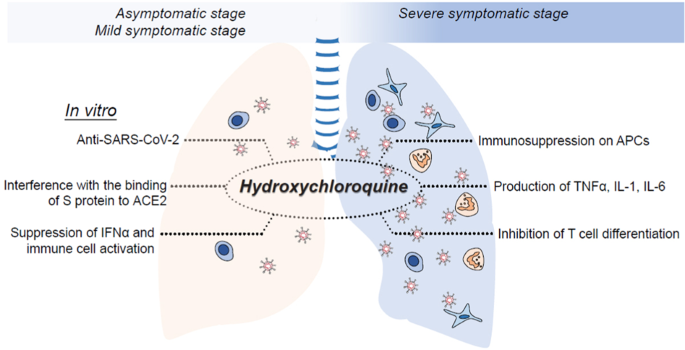
Hydroxycloroquine / Cloroquine (+ Antibiotics)
Chloroquine is a potent inhibitor of SARS coronavirus infection and spread
Severe acute respiratory syndrome (SARS) is caused by a newly discovered coronavirus (SARS-CoV). No effective prophylactic or post-exposure therapy is currently available.We report, however, that chloroquine has strong antiviral effects on SARS-CoV infection …
Observational Study of Hydroxychloroquine in Hospitalized Patients with Covid-19 | NEJM
Original Article from The New England Journal of Medicine — Observational Study of Hydroxychloroquine in Hospitalized Patients with Covid-19
Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: open label, randomised controlled trial
Objective To assess the efficacy and safety of hydroxychloroquine plus standard of care compared with standard of care alone in adults with coronavirus disease 2019 (covid-19). Design Multicentre, open label, randomised controlled trial. Setting 16 government designated covid-19 treatment centres …
Notably, the May 22 2020 release study (below) appeared to be in context of high dose HCQ on the order of 600 to 780 mg per day whereas malaria dosages are 200 to 400 mg per week. Lupus and arthritis doses 200 to 400 mg per day. Maybe less is more? More research on control group characteristics desirable. Patient disease severity stage not yet reviewed. Generally known from other sources that HCQ is not effective late stage and claims of effectiveness from other sources were during early stage. Review incomplete, but results of this study looks like high dosages are likely harmful, possibly even to patients with healthy hearts. HCQ well known to be contra-indicated when patient on beta blockers or other heart health issues – prescription only even for malaria and lupus use. Is there a study of low dose use such that heart health is less impacted? While there is still some potential that HCQ is helpful in low doses in early infection stages, the comic relief we may want to consider is in the following video segment. Again, there may be some place for HCQ in COVID-19 treatment (prophylaxis?) but enjoy the needed humor relief indicating it does not appear to be as promising as once thought.
Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis
We were unable to confirm a benefit of hydroxychloroquine or chloroquine, when used
alone or with a macrolide, on in-hospital outcomes for COVID-19. Each of these drug
regimens was associated with decreased in-hospital survival and an increased frequency
of ventricular arrhythmias when used for trea…
Hydroxychloroquine (Oral Route) Proper Use – Mayo Clinic
Drug information provided by: IBM Micromedex
It has been interesting seeing all the debate. With daily dosages in the studies on the order of 600mg and larger initial loading doses and observed that HCQ half-life is ~ 40 days, and compared that with malaria dosage, even lupus dosage, it is understandable that very sick people were getting sicker in many of the studies. Toxic / excess usage of anything is problematic. “clinical series suggest that 4g of hydroxychloroquine is potentially fatal in adults” Here’s a sad story: https://www.medintensiva.org/en-hydroxychloroquine-potentially-lethal-drug-articulo-S2173572717300577
The key to defeating COVID-19 already exists. We need to start using it | Opinion
Contrary to what you hear, there is clear-cut medical evidence for the efficacy of hydroxychloroquine.
And the debate continues. Two studies below were published and then retracted by The Lancet and other respected publishers.
RETRACTED: Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis
We were unable to confirm a benefit of hydroxychloroquine or chloroquine, when used
alone or with a macrolide, on in-hospital outcomes for COVID-19. Each of these drug
regimens was associated with decreased in-hospital survival and an increased frequency
of ventricular arrhythmias when used for trea…
RETRACTED: Chloroquine or hydroxychloroquine for COVID-19: why might they be hazardous?
The 4-aminoquinoline antimalarials chloroquine and hydroxychloroquine have been promoted
and sometimes used in the treatment of COVID-19, alone or combined with azithromycin,
based on their immunomodulatory and antiviral properties, despite an absence of methodologically
appropriate proof of their e…
And the debate continues.
Hydroxychloroquine rated ‘most effective’ coronavirus treatment, poll of doctors finds
An international poll of thousands of doctors rated the Trump-touted anti-malaria drug hydroxychloroquine the best treatment for the novel coronavirus. Of the 2,171 physicians surveyed, 37 per…
Early Outpatient Treatment of Symptomatic, High-Risk Covid-19 Patients that Should be Ramped-Up Immediately as Key to the Pandemic Crisis
Abstract. More than 1.6 million Americans have been infected with SARS-CoV-2 and >10 times that number carry antibodies to it. High-risk patients presenting
Treatment with Hydroxychloroquine, Azithromycin, and Combination in Patients Hospitalized with COVID-19
As of May 27, 2020, there were over 1,678,843 confirmed cases of COVID-19 claiming
more than 100,000 lives in the Unites States. (Cases in the U.S, 2020) Currently there
is no known effective therapy or vaccine. The urgent need for therapeutic agents has
resulted in repurposing and redeployment of e…
At 14 days, 24% (49 of 201) of participants receiving hydroxychloroquine had ongoing symptoms compared with 30% (59 of 194) receiving placebo (P = 0.21). Medication adverse effects occurred in 43% (92 of 212) of participants receiving hydroxychloroquine versus 22% (46 of 211) receiving placebo (P < 0.001). With placebo, 10 hospitalizations occurred (2 non–COVID-19–related), including 1 hospitalized death. With hydroxychloroquine, 4 hospitalizations occurred plus 1 nonhospitalized death (P = 0.29).” Interesting that the hospitalizations of hydroxy were reduced to <50% of placebo. . Would still like to see data from a lower dose study. This one is 800mg initial + 600mg in 7hrs + (600mg/day 4 days) appears to have a total dosage of 3800 mg which far exceeds the 2000mg FDA maximum for active malaria treatment. Would adverse effects be minimized with substantially lower dose? Seems like there may be some benefit in this study – don’t understand why conclusion says none. HCQ half-life is on the order of 40 days. Malaria prophylaxis FDA recommendation is 400 mg (310 mg base) once weekly.
Hydroxychloroquine in Nonhospitalized Adults With Early COVID-19: A Randomized Trial: Annals of Internal Medicine: Vol 0, No 0
Background: No effective oral therapy exists for early coronavirus disease 2019 (COVID-19). Objective: To investigate whether hydroxychloroquine could reduce COVID-19 severity in adult outpatients….
Hydroxychloroquine lowers COVID-19 death rate, Henry Ford Health study finds
Heads of the Michigan health system said Thursday the study found the drug “significantly” decreased the death rate of patients
MedicineUncensored
Breaking medical updates on COVID-19 without bias or censorship.
Facebook, Google/YouTube, Twitter Censor Viral Video of Doctors’ Capitol Hill Coronavirus Press Conference
Facebook removed a live video stream posted by Breitbart News earlier today, which at the time of removal was the top-performing Facebook post in the world, of a press conference in D.C. featuring frontline doctors speaking out against misinformation about COVID-19.
More Evidence Presented for Why Hydroxychloroquine Should be Made Available, in a New Court Filing by the Association of American Physicians & Surgeons (AAPS)
/PRNewswire/ — This week the Association of American Physicians & Surgeons submitted additional evidence to a federal court for why interference with…
What do we know about hydroxychloroquine?
There are studies looking at using these drugs for Covid-19 – but are they safe and do they work?
Is hydroxychloroquine beneficial for COVID-19 patients?
The outbreak of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first reported in December 2019. As similar cases rapidly emerged around the world1–3, the World Health Organization (WHO) declared a public health emergency of internationa…
States Bow to Pressure to Reverse Course on HCQ – Yated.com
As Covid-19 continues to burn its way across previously unscathed regions in the country, public pressure in ten states has forced governors and pharmaceutical boards to lift or ease restrictions on HCQ to fight the disease. Of the 44 states that had strict regulations in place since March, New York…
Hydroxychloroquine Studies Tied to Data Firm Surgisphere Retracted
Three authors involved in Lancet article that drew scrutiny said they couldn’t get full data set behind study; an article in the New England Journal of Medicine was also retracted
Surgisphere: governments and WHO changed Covid-19 policy based on suspect data from tiny US company
Surgisphere, whose employees appear to include a sci-fi writer and adult content model, provided database behind Lancet and New England Journal of Medicine hydroxychloroquine studies
HCQ continues to be hotly debated. While the safety and efficacy of HCQ is debated, it is clear that some studies appeared to have used near toxic doses with negative impact. The “Surgisphrere Scandal” that is related to Lancet and NEJM publication retractions further add to the controversy. The retracted papers related to the scandal indicated HCQ had no benefit and added potential harm. Some doctors vehemently argue for HCQ as helpful in early stages to avoid severe late stage disease. Other doctors vehemently argue against it, though less-so after the publication retractions. Most agree it is not helpful in late stage disease. While the debate should have science at the center, it often travels along political lines. Really Correct continues to follow the debate and attempts to provide multi-representational perspectives of the available information.
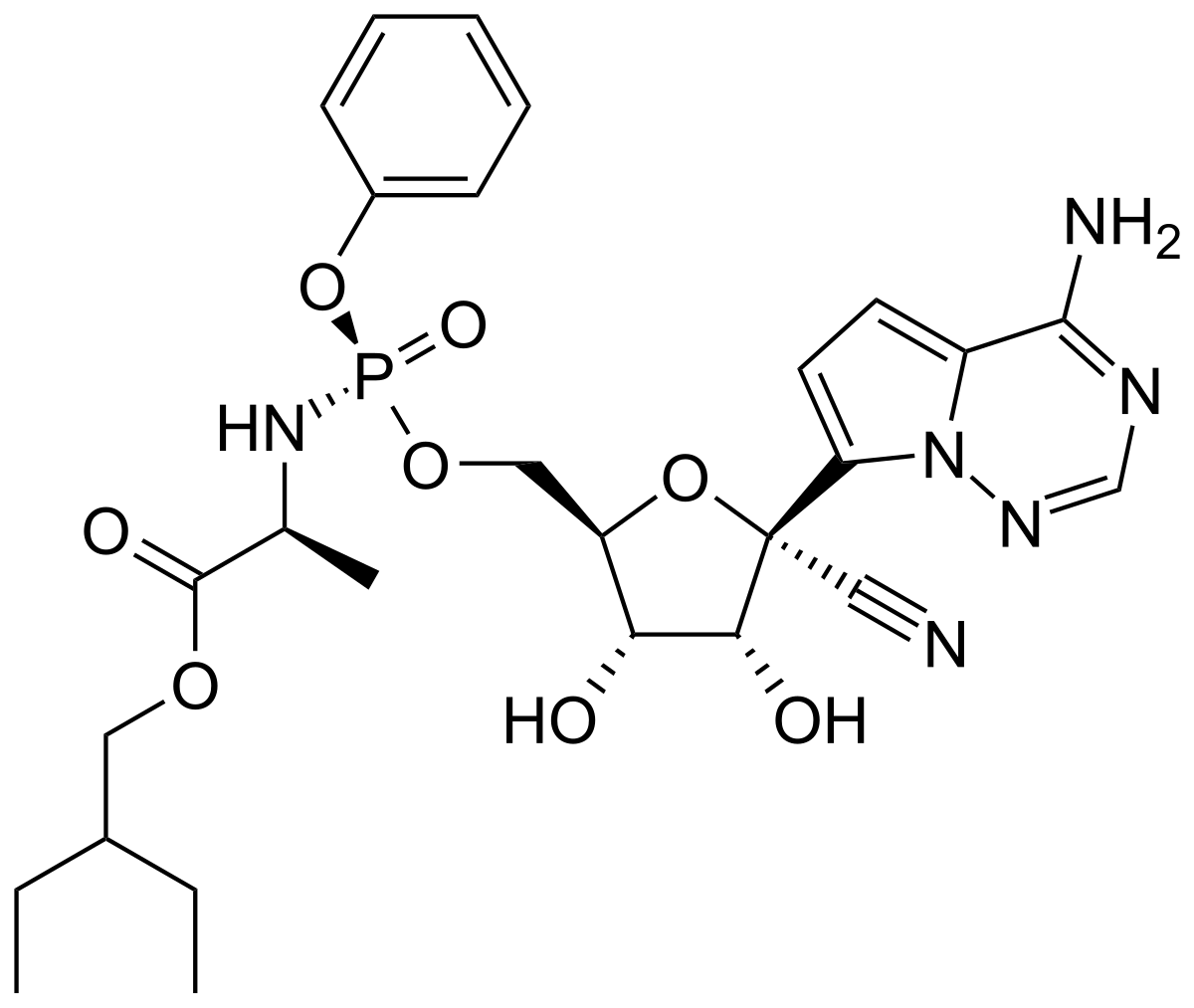
Remdesivir
Remdesivir – Wikipedia
IUPAC name
Inside the NIH’s controversial decision to stop its big remdesivir study
At the heart of the decision was a process that was — as is often in the case in clinical trials — by turns secretive and bureaucratic.
‘Clear-cut’ evidence coronavirus drug remdesivir works, Fauci says
Remdesivir, an experimental coronavirus drug from Gilead Sciences, is showing ‘clear-cut’ evidence that it works in a new study, according to Dr. Anthony Fauci.
Remdesivir for the Treatment of Covid-19 — Preliminary Report | NEJM
Original Article from The New England Journal of Medicine — Remdesivir for the Treatment of Covid-19 — Preliminary Report
PulmCrit: Remdesivir 5-day vs. 10-day trial raises some red flags?
So, Gilead’s first RCT on remdesivir was just published, and it’s very interesting.1 Gilead’s, you say? Yep. The study was designed,
Sorrento’s COVID-SHIELD (COVID-GUARD or whatever they end up calling it)
“Sorrento’s COVID-SHIELD is meant to address this through a potent mix of different antibodies that provide protection against different strains of the virus, but the company says it also will be pursuing development of the STI-1499 antibody on its own as a dedicated, standalone therapy. The company is already in discussion with regulators about how to expedite development of that potential treatment, and is ramping its production capacity as well with the goal of producing as many as one million doses at the same time it pursues FDA approval for its use.”
STI-1499, A Potent Anti-SARS-CoV-2 Antibody, Demonstrates Ability To Completely Inhibit In Vitro Virus Infection In Preclinical Studies
Sorrento Therapeutics, Inc. (Nasdaq: SRNE,
“The company plans to test whether STI-1499 prevents infection in monkeys and possibly ferrets — two species that are susceptible to the virus. If all goes well, Sorrento Therapeutics could begin testing the antibody in clinical trials of severe COVID-19 patients by mid-July, Ji says.”
San Diego’s Sorrento Therapeutics says antibody might have ability to fight COVID-19
The biotech company is preparing to make the protein part of a cocktail to battle the virus
Sorrento finds a coronavirus antibody that blocks viral infection 100% in preclinical lab experiments
Therapeutics company Sorrento has made what it believes could be a breakthrough in potential treatment of SARS-CoV-2, the virus that leads to COVID-19. The company released details of its preclinical research on Friday, announcing that it has found an antibody that provides
Sorrento Therapeutics’ stock soars on massive volume after upbeat report on COVID-19 antibody experiment
Shares of Sorrento Therapeutics Inc. undefined blasted 153% higher on very heavy volume in afternoon trading Friday, putting it on track to close at a near…
Covid Report: Tiny Biotech Sorrento Claims It Has A Coronavirus Cure
When you’re trying to find the best stocks and identify the right time to buy them, there are three key pieces to that investing puzzle: Overall market conditions, the company’s fundamental strength, and the chart action. The biggest gains – and the least risk – come when you have positive indicator…
Mesenchymal
Mesenchymal Stem Cell Therapy for COVID-19: Present or Future
“COVID-19” is the word that certainly isn’t forgotten by everybody who lives in the first half of the twenty-first century. COVID-19, as a pandemic, has led many researchers from different biomedical fields to find solutions or …
ECMO
Critically Ill COVID-19 Patient Better After ECMO Treatment
Experts offer guidance on ECMO use in pandemic setting
Cytokine Adsorption
Cytokine Adsorption in Severe COVID-19 Pneumonia Requiring Extracorporeal Membrane Oxygenation – Full Text View – ClinicalTrials.gov
Cytokine Adsorption in Severe COVID-19 Pneumonia Requiring Extracorporeal Membrane Oxygenation – Full Text View.
HIV Meds
Why Do Researchers Think HIV Meds Might Work Against COVID-19?
At least one such drug still holds that promise against coronavirus, but in general there’s little precedent for the same drug blocking different viruses.
“But then lopinavir/ritonavir failed against COVID-19 in a decently sized study in China. While there are still other trials planned to investigate this medication, many lost hope in its promise after news of this study broke.”
An article discussed HIV meds being a possible therapy because some studies of HIV patients with SARS or COVID led a researcher to believe they helped. A hypothesis exists such that better outcomes were not the HIV meds, but the fact that the patients were HIV+ and had lower cytokine production due to lower CD4 T-helper cell counts (or something like that). Is it possible that HIV+ have lower risk of cytokine storm related COVID-19 morbidity? Does this point to some potential therapy areas and/or the genesis of SARS-CoV-2 virus RNA changes? Also see Hypotheses
Thrombotics
COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up
Coronavirus disease 2019 (COVID-19), a viral respiratory illness caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), may predispose patients to thrombotic disease, both in the venous and arterial circulations, due to excessive …
Drug treatments for covid-19: living systematic review and network meta-analysis
Objective To compare the effects of treatments for coronavirus disease 2019 (covid-19). Design Living systematic review and network meta-analysis. Data sources US Centers for Disease Control and Prevention COVID-19 Research Articles Downloadable Database, which includes 25 electronic databases and…
Identification of Antiviral Drug Candidates against SARS-CoV-2 from FDA-Approved Drugs
Drug repositioning is the only feasible option to immediately address the COVID-19 global challenge. We screened a panel of 48 FDA-approved drugs against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) which were preselected by an assay of SARS-CoV. We identified 24 potential antiviral …
Hospitalized COVID-19 patients treated with Convalescent Plasma in a mid-size city in the midwest
Background SARS-CoV-2 and its associated disease, COVID-19, has infected over seven million people world-wide, including two million people in the United States. While many people recover from the virus uneventfully, a subset of patients will require hospital admission, some with intensive care need…
FROM NYC ICU: DOES COVID-19 REALLY CAUSE ARDS??!!
I am a physician who has been working at the bedside of COVID+ patients in NYC. I believe we are treating the wrong disease and that we must change what we a…
Do COVID-19 Vent Protocols Need a Second Look?
For full transcript, reference, and resources: https://wb.md/2Xprogq Welcome to
PulmCrit – Is COVID-19 ARDS, pseudoARDS, L, or H? Physiology data from Boston
There has been considerable speculation in the literature regarding the physiology of intubated patients with COVID, but little actual data. A fresh
Startling images reveal coronavirus forming tentacles in cells. It may help identify new treatments.
Researchers also identified a family of existing drugs that may be the most effective yet in treating patients with COVID-19.
Inside the Coronavirus
What scientists know about the inner workings of the pathogen that has infected the world