Partial List Of Epidemic Risk Management Methodologies
- Isolate High-Risk Population And Minimize Infection Window Period
Minimize the period where infection is actively spreading and isolate high-risk population during that time. - Complete Containment
Use all available means in attempt to create virtually zero viral transmission - Delay Until Treatment Options Improve
Apply Safety Protocols while preparing treatment best practices - Delay Until Vaccine Available
Apply Safety Protocols until vaccine becomes available - Ensure Medical Facility Availability
Modulate Safety Protocols as needed to ensure medical facility availability
Each of the various Epidemic Risk Management Methodologies have differing trade-offs. The sections that follow identify and define the various methodologies. Some areas which are impacted differently by different methodologies include:
- Sickness and death of high-risk population
- Sickness and death of low-risk population (by definition, low-risk population rarely experiences high-severity or death)
- Economic impact (business, personal income, supplier payments, housing / rent, etc.)
- Social health impact (relationships / family, recreation, elderly relationships, suicide, etc.)
- Social structure impact (government, constitutional crises, social unrest, riots, crime, murder)
Minimize Infection Window Period
Minimize The Time Period That The Infection Is Rapidly Spreading. This approach can minimize the impact on high-risk populations as the infection probability window is reduced in time. In this approach, the high-risk population remains strongly isolated while the low-risk population continues day to day activity; keeping economic and social structures largely intact. As a result, many of the low-risk population are more likely to become infected much more rapidly than if the low-risk population follows safety-protocols. The low-risk population becomes infected, recovers, and gains whatever immunity may be associated with their immune system having acted to recover from the initial infection. At some point enough of the low-risk population completes the cycle such that the virus no longer can find hosts in which to replicate and the virus then largely ceases to exist. Any remnants on surfaces eventually become inactivated by UV, heat, and other naturally occurring activity and/or intentional cleaning activity. After the virus is virtually removed from circulation, the high-risk population can safely emerge from isolation. It is often important to also ensure medical facility availability.
Additionally, studies have demonstrated that low viral load exposures caused people to develop increased immunity levels without becoming significantly sick – they “seroconverted while having minimal clinical illness and no shedding“.
Since the low-risk population completes this cycle rapidly, the high-risk population has a smaller time window in which it must remain isolated. Also, for those who have recovered, immune response to re-exposures are more rapid the closer that re-exposure is to the time when recovery occurred; which further limits transmission probability.
The economic, social health, and social structure impacts tend to be very low for the vast majority of the population.
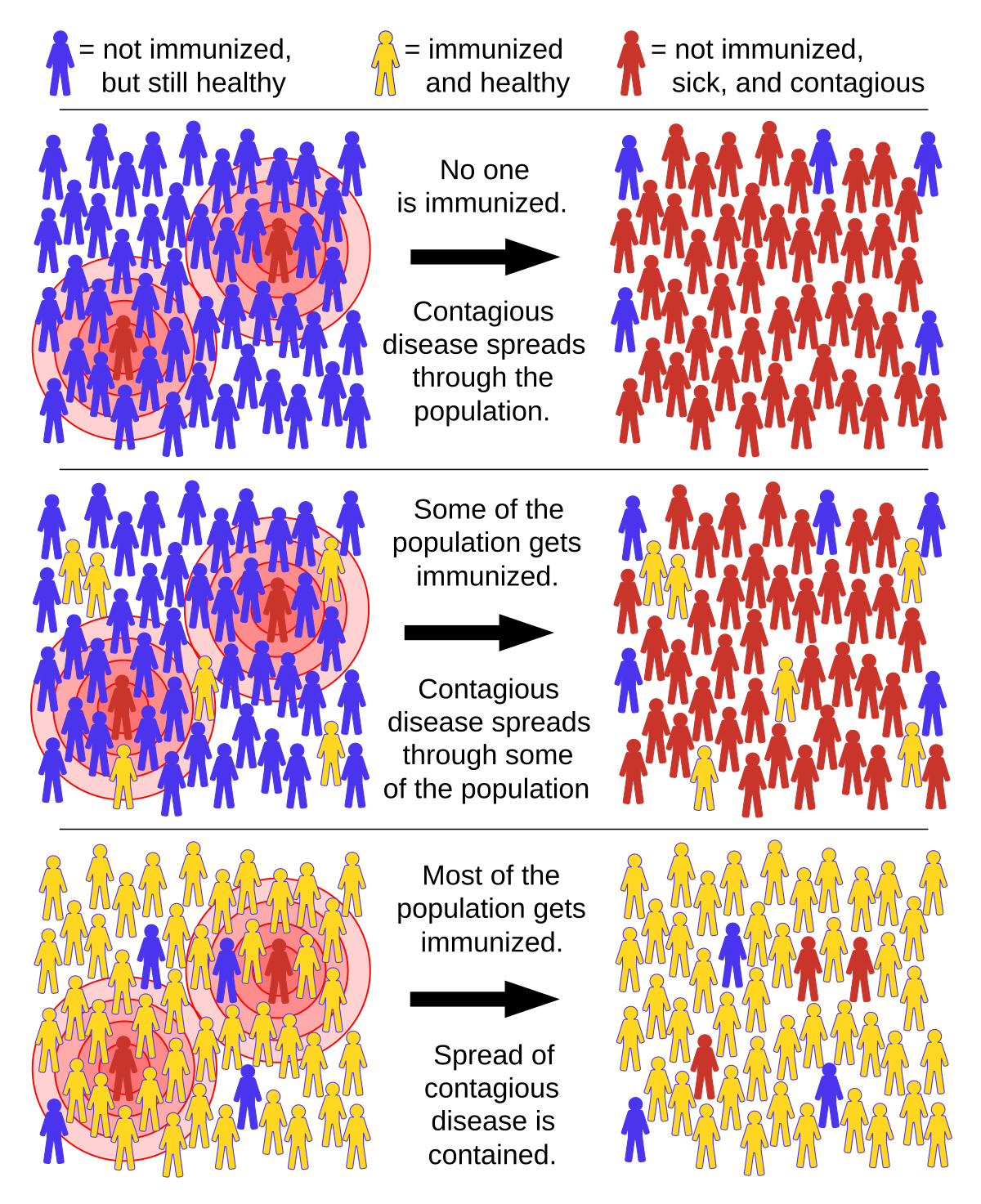
This process is built upon the idea that individuals who cannot be infected are not good hosts for the virus and do not enable the virus to replicate and therefore do not shed viruses. It has been shown that “The greater the proportion of immune individuals in a community, the smaller the probability that non-immune individuals will come into contact with an infectious individual, helping to shield non-immune individuals from infection.”
While those caring for uninfected high-risk populations may be able to isolate themselves, forgo normal social activities, and remain dedicated to protecting their high-risk family and clients / patients, they will eventually compromise or make errors that expose themselves to infection, thus exposing the high-risk group. Minimizing the infection window period minimizes the chance of human error and helps those caring for high-risk populations get back to normal life sooner.
Some people refer to this concept as “Herd Immunity” but that term can have multiple definitions. One definition is “virtual eradication”. Another definition views Herd Immunity as an analog phenomenon where more immune help protect those not immune on a variable scale such that every person that gains immunity reduces the probability that others will become exposed. Also, when considering concepts of herd-immunity, it is important to recognize that a percentage of the population is low risk for exposure and transmission due to “reclusive” social habits. It has been observed that in recent decades, there has been a trend toward significantly lower social interaction. The largely-isolated population, which may be on the order of 30%, could be directly subtracted from the total population for use in herd-immunity calculations. For example, if 20% of the population was found to be immune, the herd-immunity level, when adding 30% “homebodies”, may result in an effective herd-immunity on the order of 50%. During a pandemic, fear may even increase the socially isolated population.
Diseases with extremely high consequences, sequelae, and fatality rates require virtual eradication to protect the population. Diseases with extremely low consequences require no special care except that which minimizes the inconvenience of being sick. Diseases with consequences between these extremes need commensurate risk management protocols, and thus are managed on an analog scale rather than extreme prevention measures or zero measures to prevent transmission. This approach of “natural immunity” is perhaps obviously not favorable with diseases of high-consequences to a large population percentage. That threshold is a subjective decision that must be balanced against other societal factors.
For example, measles has been stated to have a Infection Fatality Rate (IFR) of 15% and neurological damage rate of 25%. It is understandable why this may create a desire for complete eradication. The average Seasonal Flu has a IFR of about 0.1% (in some years as high as 0.3%) and is generally considered survivable to most of the general population; vaccines have been partially effective at reducing seasonal flu and it is generally considered as not requiring eradication though some segments continue to push for perfect vaccines. As of June 2020, the CDC models COVID-19 with a 0.4% Infection Fatality Rate. Significant sequelae for COVID-19 have been found in hospitalized patients, particularly those who were placed in invasive ventilation (intubation). However, the vast majority of mild-cases, especially those unreported, are not presenting any significant sequelae as it would be expected that the tens of millions US recovered population to be seeking medical attention if sequelae following mild cases were common-place.
Complete Containment
Use All Available Means In Attempt To Create Virtually Zero Viral Transmission. This option can rarely achieve sufficient isolation to halt an epidemic. When a geographic area can be fully isolated until the geographic areas with active infections drop to virtual zero, this may be possible. The group not being infected will gain no immunity to the pathogen or any immunologically similar future mutations. The uninfected group will have virtually no casualties or impact from the virus itself during the period where the virus does not enter that group. Future infection is likely after containment ends. Often, complete containment results in an outbreak that is deferred rather than avoided. Additionally, attempts to contain an outbreak can also inhibit repeat exposure to those who have already recovered; thus negatively impacting their long-term immunity. Repeat exposure is known to often result in both stronger and longer immunity. The economic, social health, and social structure impacts tend to be very high and may have multi-year, and potentially permanent, effects.
Highly infectious pathogens, such as SARS-CoV-2, rarely can be contained, only slowed. Attempting to completely contain SARS-CoV-2 with current technology in the US and many other countries has proven to be a fool’s errand. Many other pathogens such as the common-cold (which is also a type of coronavirus) are also too infectious to stop. Slowing spread and management are possible, but complete containment is rarely a realistic option for large land mass areas. Beginning in March 2020, virtual COVID lockdowns began and continued for 1 to 3 months in various US states. This shutdown failed to contain the outbreak which is believed to have entered in the US in December 2019 or earlier when most countries were equally unaware of growing infection rates. Some of the earliest reports of numerous cases in the US and Europe were linked to ski resorts with infection numbers far beyond many timelines in the links above. This suggests that COVID had been circulating within the US and Europe in January 2020 or earlier. It is likely that many skiers were at low-risk for severe cases and thought they had a flu in the months before COVID became common knowledge. Containment of pathogens that result in mostly non-severe, flu-like symptoms, is extremely challenging as the earliest infections tend to among the socially mobile, active, and low-risk for severe-case population; and thus tend to be unreported.
Delay Until Vaccine Available
Use All Available Means In Attempt To Create Virtually Zero Viral Transmission Until A Vaccine Is Available. The economic, social health, and social structure impacts tend to be very high and may have multi-year, and potentially permanent, effects.
If a vaccine is readily available, those willing to use it can reduce the infectable population. Without a vaccine, those at low-risk to severe complications might choose to take the risk of becoming infected, recovering, and gaining whatever immunity may be associated with their immune system having acted to recover from the initial infection which also can reduce the infectable population.
Delay Until Treatment Options Improve
Use more aggressive Safety Protocols Until Treatment Options Stabilize. Depending upon the delay and severity of safety protocols, the economic, social health, and social structure impacts tend to be very high and may have multi-year, and potentially permanent, effects. This approach can attempt to find a balance between delay and improved treatment options.
During the first month of COVID-19 in the US, some treatment options were found to cause increase fatality rate. Two areas that were particularly problematic were premature use of invasive intubation ventilation and excessive ventilation pressure. Other treatment problems currently under investigation included excess doses of steroids and HCQ in severe patients – as use case for both of these therapeutics targeted low-dose and early use. Using more aggressive Safety Protocols can be helpful during the period where treatment options are being rapidly improved. Emphasis on transparency and sharing of treatment options can increase the speed at which poor treatment approaches are eliminated.
Ensure Medical Facility Availability
Use more aggressive Safety Protocols Only When Medical Facility Availability Is Threatened. This management approach seeks to model the epidemic and predict when medical facilities will become severely stressed and uses commensurate means to ensure medical facilities remain available. It also involves surge capacity planning that may include use of hospital ships, mobile facilities / RV’s, and ad-hoc tented triage areas. This approach is often a sub-component of other approaches. “If individuals and communities take steps to slow the virus’s spread, that means the number of cases of COVID-19 will stretch out across a longer period of time.“. In any outbreak, there is likely an optimum time period where infections occur slowly enough that medical facilities are not overwhelmed but infections occur rapidly enough so as not to extend the outbreak time period.
Summary
All of this is an attempt to balance an equation. When listing the various options available, there exist different advantages and disadvantages for each option that might be selected. To evaluate the disadvantages of only one option does not enable the equation to be balanced. While enough data may exist to determine an optimal solution at this time, it is more likely that it may be necessary to take several approaches based on voluntary participation and freedom of individual choice – and then observe in retrospect the results of those competing choice selections. This may be the only way to obtain all of the data needed to make better choices in the future. This approach of informed personal liberty and discretion may also create opportunity for intuitive, common-sense, choices that are baked into human behavior that are not well documented or formalized in studies. As one anecdotal example of intuitive behavior, during early beach re-openings in California, it was observed that many kinship groups remained about 20 to 50 feet apart, even though a formal rule was 6 feet. This was observed along two separate 4-6 mile stretches of beaches in two different California counties – showing some clear, common, instinctive behavior among diverse groups outside of shared visual range. As more heavy-handed measures increased due to some small number of violations, there appeared to be a greater tendency for many groups to be larger and tighter in apparent defiance of the increased measures. Human psychology creates interesting interplay between intuition, data, and attempts at control.
Reference Material





With COVID-19 case numbers climbing dramatically in the United States and millions of people sheltered in their homes to help quell the outbreak, many are asking the obvious question: How long will all this last? Yale School of Public Health Associate Pr…



People at high risk for serious cases of COVID benefit when low-risk populations become immune.

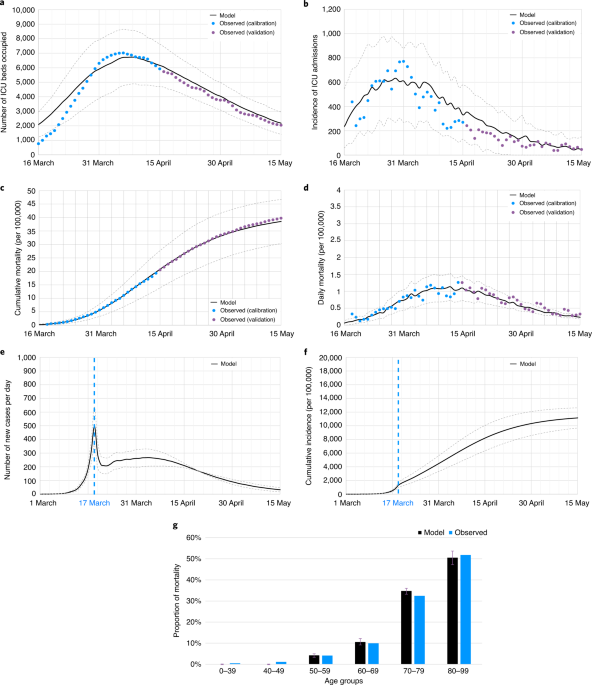
“While lockdown is effective in containing the viral spread, once lifted, regardless of duration, it would be unlikely to prevent a rebound. Both physical distancing and mask-wearing, although effective in slowing the epidemic and in reducing mortality, would also be ineffective in ultimately preventing ICUs from becoming overwhelmed and a subsequent second lockdown. However, these measures coupled with the shielding of vulnerable people would be associated with better outcomes, including lower mortality and maintaining an adequate ICU capacity to prevent a second lockdown.”